Movement: the foundation
of functional capacity
and sustainable prevention
Movement is central to human development and the functional balance of the body.
Understanding its biomechanical and neuromotor mechanisms helps explain the onset of compensations, chronic pain, and musculoskeletal disorders.
In modern societies characterized by sedentary lifestyles and repetitive positions, movement has become a public health issue and a factor in sustainable performance.
This page offers a structured overview of the movement: from its initial development to its alterations, and its central role in the prevention of MSDs.
Summary

Movement as a system
neuro-biomechanics
Movement is not simply a matter of displacement.
It corresponds to coordinated organization between:
The central nervous system, which plans and adjusts action
Joint structures, which determine possible ranges of motion
Muscle chains, which produce and regulate force
Each gesture simultaneously involves several dimensions:
Gross motor skills: movements and actions involving the whole body (walking, running, jumping)
Fine motor skills: precise coordination of the distal segments (writing, grasping, manipulating)
Axial movement: flexion, rotation, and trunk inclination
Specific joint mobility: local expression of a joint in its optimal range of motion
These components operate in constant interaction.
The quality of the movement depends on their synchronization.
When one of them is altered, the overall balance changes and compensatory strategies emerge.

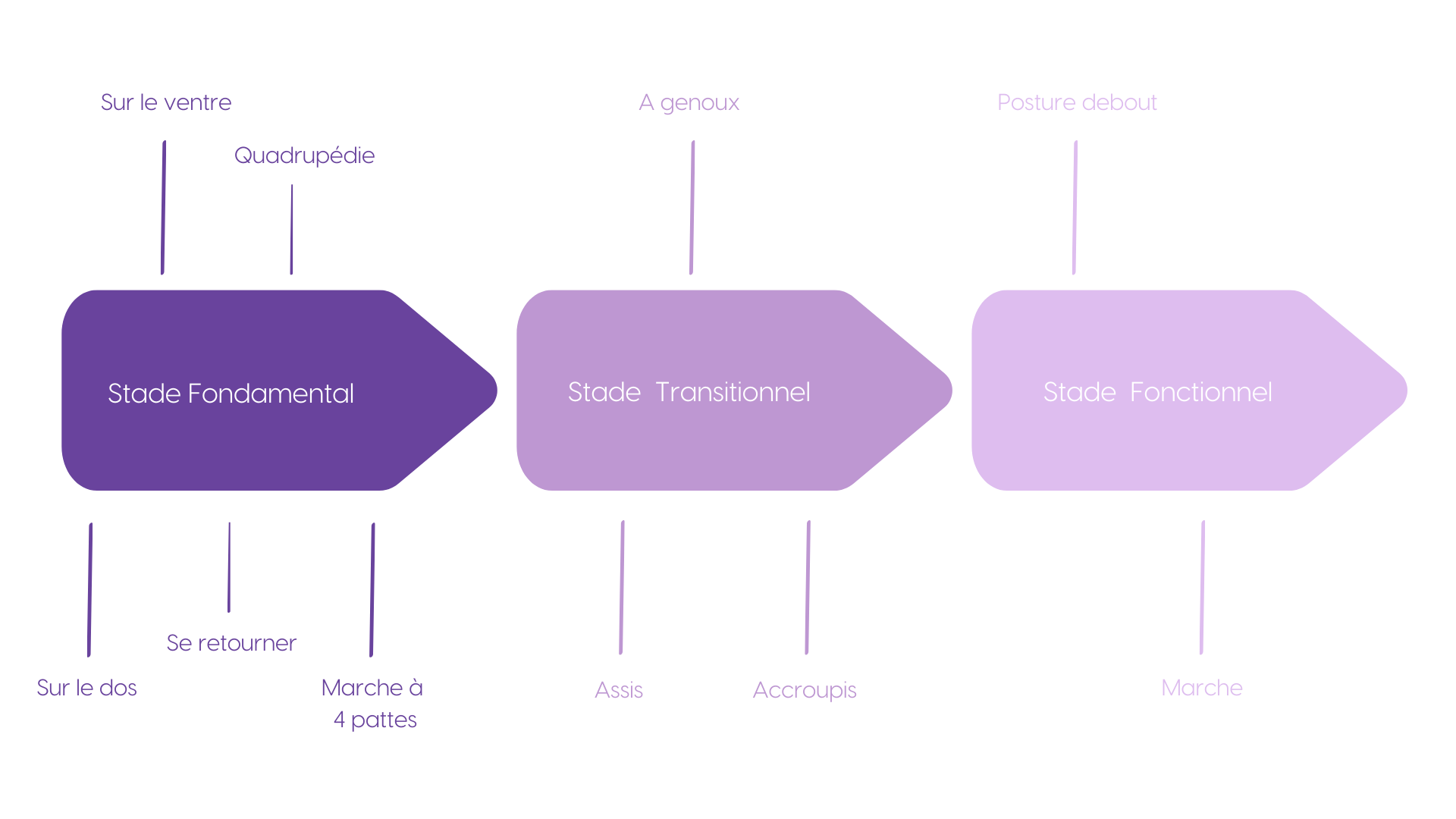
Motor development:
from birth to independence
At birth, the dominant muscle activity involves the anterior chains.
They keep the infant in a flexed, inward-facing position.
Gradually, under the influence of sensory stimulation (visual, vestibular, proprioceptive), the child organizes its recovery: head control, rolling over, crawling, crawling on all fours, sitting up, then standing up.
During these stages, the posterior chain develops and enables extension, alignment, and verticalization.
By the age of three, the major fundamental motor patterns are consolidated and reach a high level of spontaneous efficiency. Neurological plasticity remains significant, but the motor skills are in place.
Then, gradually, a sedentary school lifestyle sets in, marking the beginning of a reduction in daily motor variability.
A natural imbalance amplified by modernity
The human body has a biomechanical structure that is primarily geared towards flexion.
Schematically, we observe:
Approximately two-thirds of the muscle forces directed forward
One-third backward
This predominance can be explained by the function of the anterior chains, which are heavily involved in grasping, exploring, and performing actions.
When mobility is preserved and there is sufficient range of motion, this balance poses no problem.
On the other hand, in static environments, where people are mainly seated and facing forward, repeated stress on the flexion chains gradually accentuates this imbalance.
Added to this is a physiological phenomenon: as we approach the age of 40, muscle mass and strength gradually decline in the absence of appropriate stimulation.
Adaptability is declining.
The risk of compensation increases.
2/3 of force directed forward
1/3 of force directed backward
When moving, this relationship remains functional.
During prolonged sedentary periods, posterior capacity declines,
and balance is disrupted in favor of forward flexion.
The fundamental equation of motion
Efficient movement relies on three inseparable components:
HEALTHY MOVEMENT = MOBILITY × STABILITY × MOTOR CONTROL
Mobility
The ability of a joint to express its optimal range of motion while respecting its biomechanical axes, particularly in rotational areas such as the shoulder or hip.
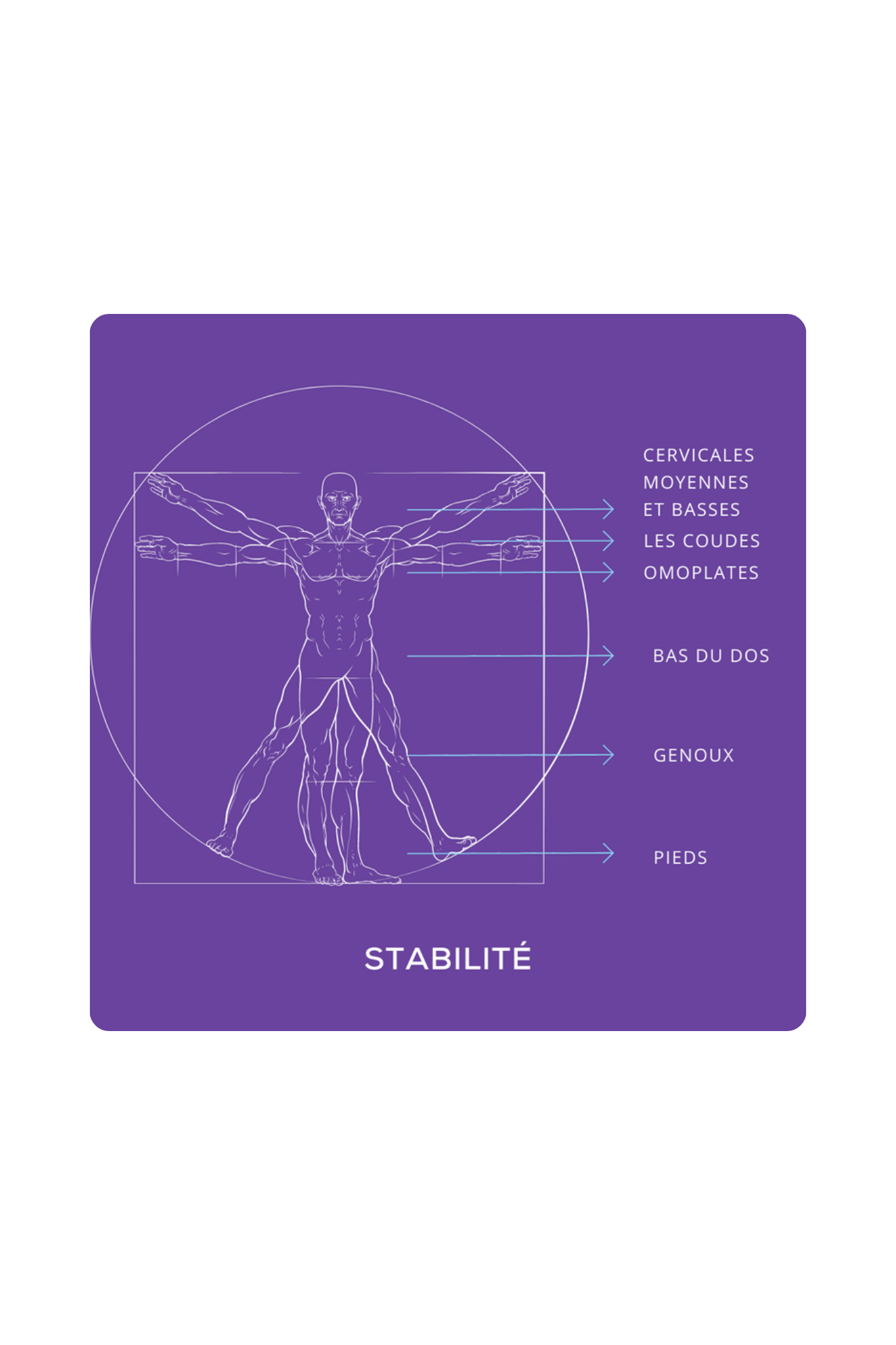
Stability
Ability to create segmental anchoring that allows for the effective transmission of forces, particularly at the knee and lumbar spine.
Engine control
Organization and selection of motor patterns by the central nervous system. These patterns, derived from experience, are activated and adjusted in real time during the execution of a movement.
We distinguish between:
open-loop diagrams (preprogrammed)
closed-loop patterns (adjusted by sensory feedback)
They constantly evolve depending on repetition, fatigue, and context.
A change in just one of these factors alters the mechanical quality of the overall movement.
Posture and movement:
an inseparable dynamic
Opposing posture and movement is a simplification.
Movement corresponds to a continuous transition:
Starting position → segmental activation → final position.
Even when standing still, postural muscle activity is regulated by constant tonic adjustments.
Absolute immobility does not exist.
Effective posture is never static.
It is dynamic, adaptable, and dependent on the quality of motor control.
Improving posture necessarily involves improving movement.
These mechanisms make perfect sense in a structured prevention approach within a company.
Repetitive positions: silent enemies of movement
The musculoskeletal system is designed for variability.
When we maintain a prolonged position and/or perform repetitive movements:
Muscle activity becomes asymmetrical
Some structures are underutilized.
Others experience cumulative stress
The lack of movement variability reduces tissue adaptability.
Imbalances are emerging.
These adaptations, known as compensations, cause the nervous system to gradually modify its motor patterns.
This mechanism can lead to:
Joint stiffness
Overloading of other segments
A gradual reduction in amplitude
A fear of movement (kinesiophobia)
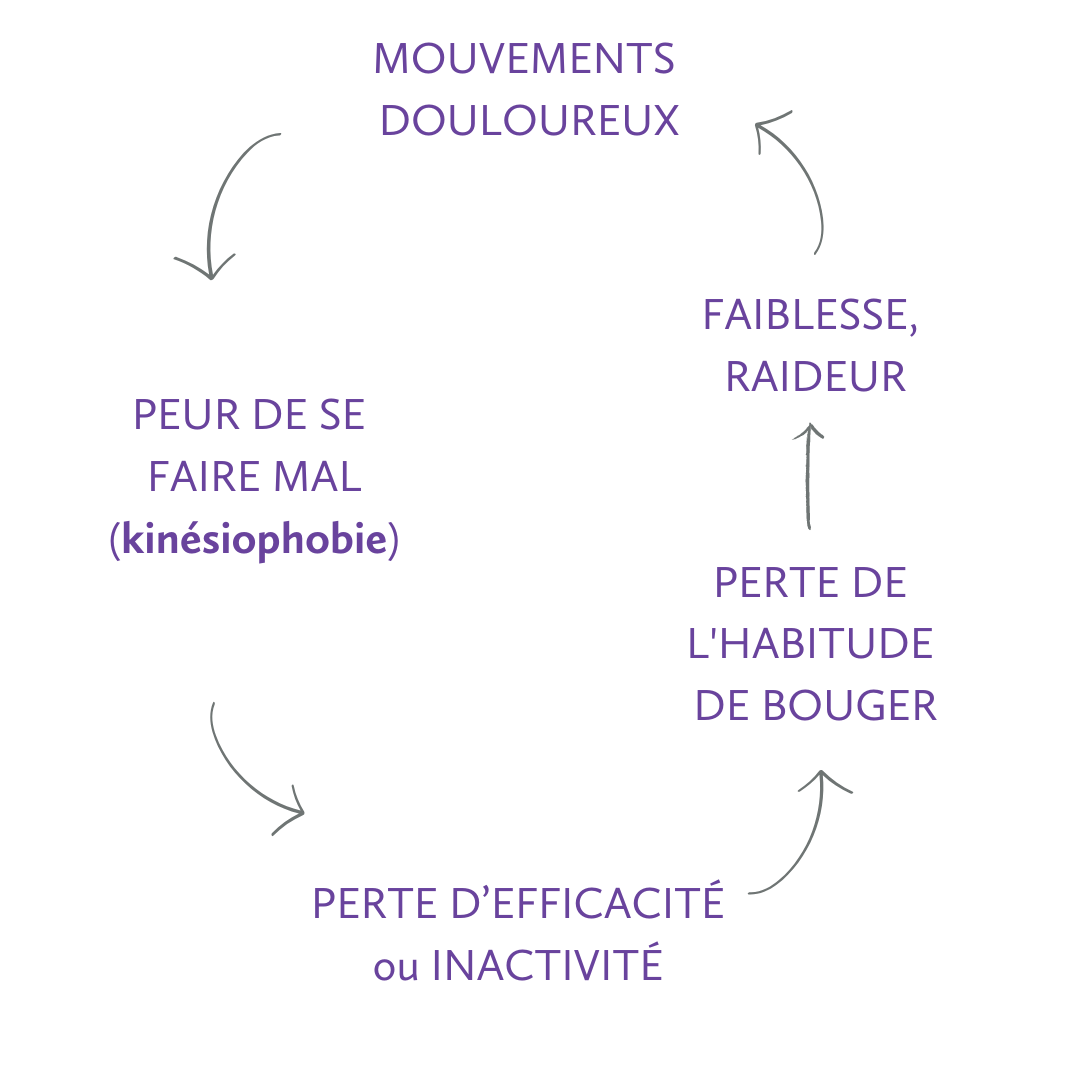
The vicious cycle of kinesiophobia
Common examples of repetitive positions: Prolonged sitting, Prolonged standing, Repeated use of a mouse, Long periods of driving, Intensive use of a smartphone, etc.
Compensation and alteration of motor patterns
Let's take the example of the thoracic region, which is physiologically designed for rotation.
When sitting for long periods:
The posterior chain relaxes
The rib cage loses mobility ( upper back)
Rotation becomes limited
The nervous system (motor control) redistributes the stress to adjacent segments. The cervical or lumbar region, which is less suited to repeated dominant rotation, is subjected to greater stress.
This change in the axes of movement results in:
A local increase in tissue stress
A gradual deterioration in mechanical efficiency
In the long term, chronic pain or structural damage may occur.

When a mobile area becomes "stiff," a stable area is forced to compensate to provide the missing mobility.
Movement and
musculoskeletal disorders
Musculoskeletal disorders (MSDs) include damage to the tissues of the musculoskeletal system: muscles, tendons, tendon sheaths, joints, and, in some cases, spinal structures.
In business, they are favored by a combination of constraints:
repetitive movements and high speed
prolonged postures, especially outside neutral zones
efforts, handling, vibrations
insufficient recovery and low movement variability
organizational and psychosocial constraints, which can increase baseline muscle tension
The link with movement is central: MSDs are not only related to external constraints, but also to the gap between imposed constraints and functional capacity (available mobility, stability, motor control, local endurance).
When the quality of movement deteriorates, the distribution of loads changes: certain areas become overworked, recovery is incomplete, and repeated micro-overloads can lead to the onset of pain and then to lasting damage.
The most common locations are:
upper limbs
cervical region
lumbar region
A detailed analysis of the mechanisms behind the onset of MSDs in the workplace provides insight into their organizational and regulatory implications.
Learning to move again: restoring balance
An altered motor pattern does not correct itself spontaneously.
It requires gradual exposure, controlled repetition, and conscious adjustment. This approach involves an initial assessment, structured monitoring, and protocols tailored to each individual's functional profile.
The process can be described in four steps:
Unawareness of the deficit
Awareness through evaluation
Voluntary reorganization of movement
Automated integration through repetition
A rebalanced movement:
Limits compensation
Improves postural ability
Optimizes force transmission
Reduces the risk of MSDs
Movement is not limited to physical activity.
It is the dynamic expression of human functional capacity.
When mobility, stability, and motor control are balanced, the body effectively absorbs stress. When they are impaired, compensatory strategies take over.
Understanding these mechanisms makes it possible to structure sustainable prevention of musculoskeletal disorders and ensure long-term functional health.